Pain relief is one of the most important functions of an ED. Pain is the primary presenting symptom in over 50% of ED attendances and should be managed in a timely fashion.
Acute Severe Pain.
The gold standard is intravenous morphine in boluses of 5mg titrated to effect. This should be reduced in the elderly 1-2mg boluses. The dose for children is 0.1- 0.2 mg/kg. There is no role for the intramuscular route. There is no need to routinely give an anti-emetic unless the patient is already vomiting
Mild to Moderate Pain.
This can usually be treated with oral analgesia. See table below. Diclofenac 100mg PR is a very effective analgesic.
Discharge Analgesia Most patients with soft tissue injuries can be managed with OTC analgesia such as Paracetamol or Ibuprofen. The next step should be Diclofenac or Paracetamol/ Codeine 500/30 (Solpadol/Tylex). There is no role for Tramadol in the ED.
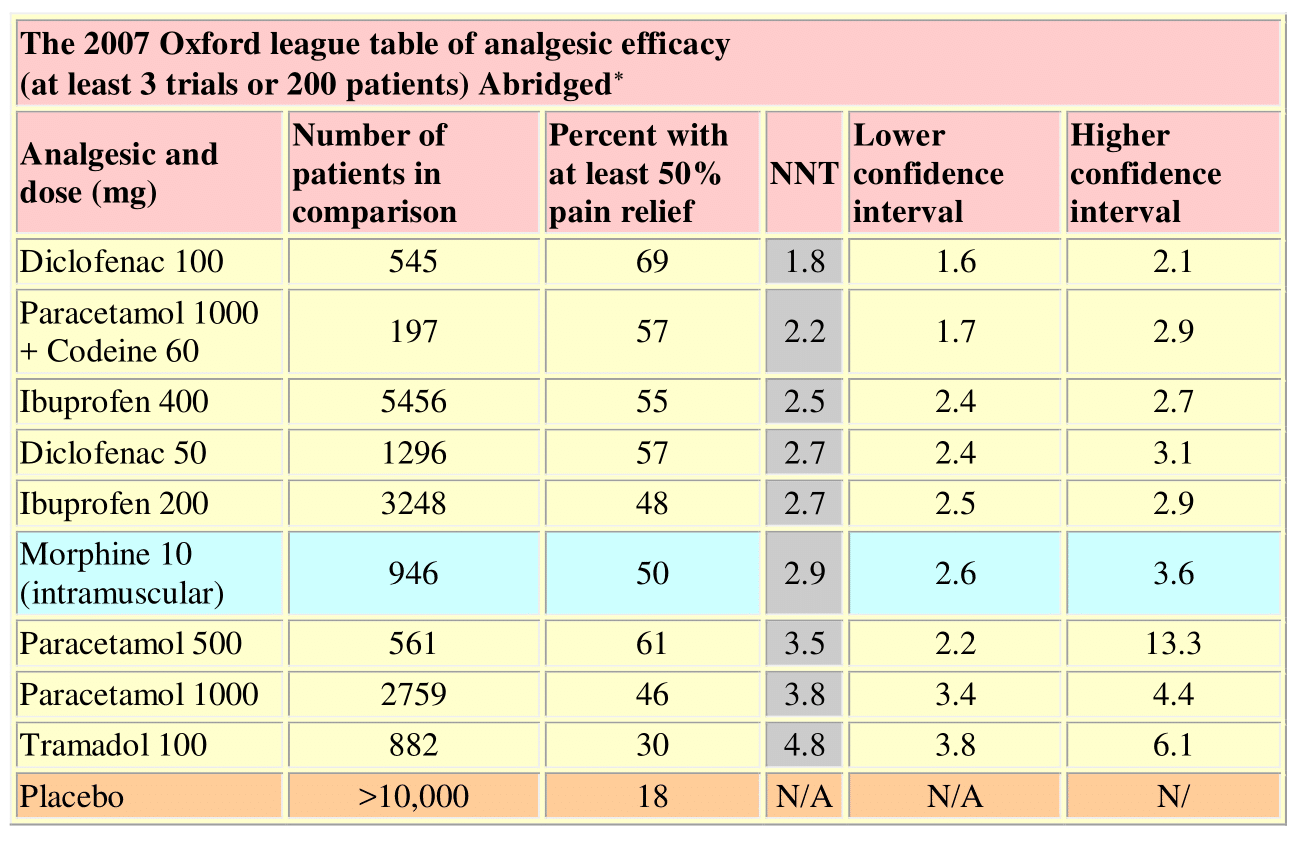
Numbers needed to treat are calculated for the proportion of patients with at least 50% pain relief over 4-6 hours compared with placebo in randomised, double-blind, single-dose studies in patients with moderate to severe pain. Drugs were oral, unless specified, and doses are
milligrams. Shaded rows are intramuscular administration